The percentage of oncology patients participating in clinical trials is remarkably low: 8.1 percent according to a recent meta-analysis. While this is more encouraging than the commonly cited value of 3 percent, it is nonetheless disappointingly low and explains the daunting recruitment challenges that sponsors face in most oncology trials.
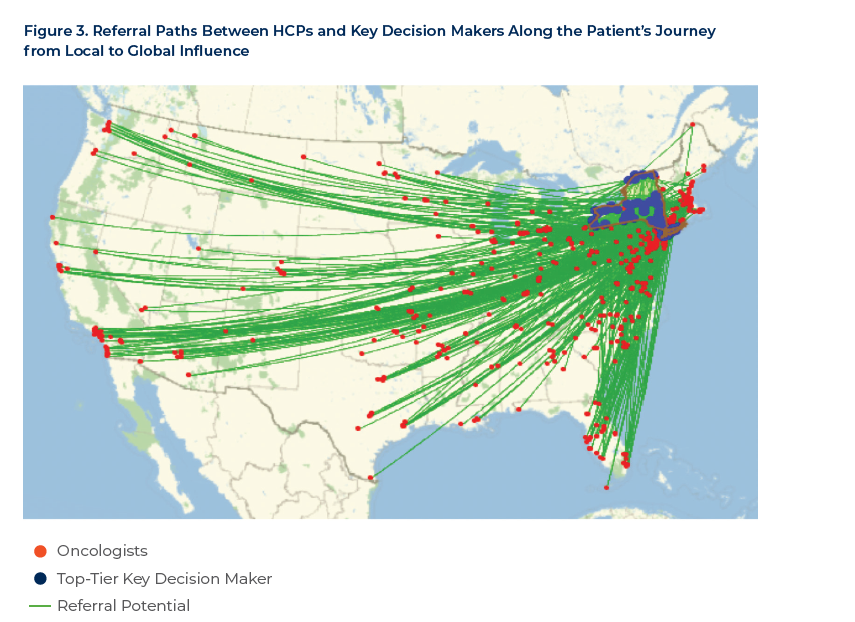
Low participation rates are largely attributed to access issues (the availability of trials in the right geography for a given cancer type or stage) and eligibility restrictions. However, a number of other factors often compound the situation, including a heavy patient burden (in terms of clinic visits, tissue sampling requirements, etc.), patient misconceptions concerning trials, lack of awareness on the part of patients and physicians, and a failure to reach patients with study information at the right time in their treatment journey.
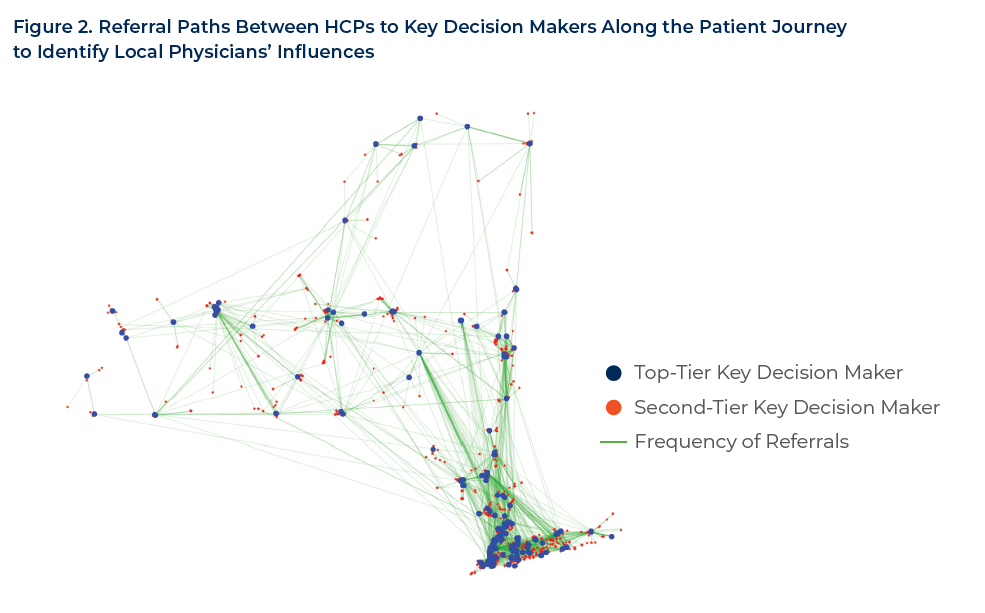
Cancer patients frequently rely on their physicians to inform them of trials for which they might be eligible. Meanwhile, many investigators appear to wait for the ideal study participants to walk through their door at just the right time in their treatment progression. As a result of these two factors, which ultimately leave a key aspect of patient recruitment to chance, it is little wonder that most trials experience delays due to slow enrollment.
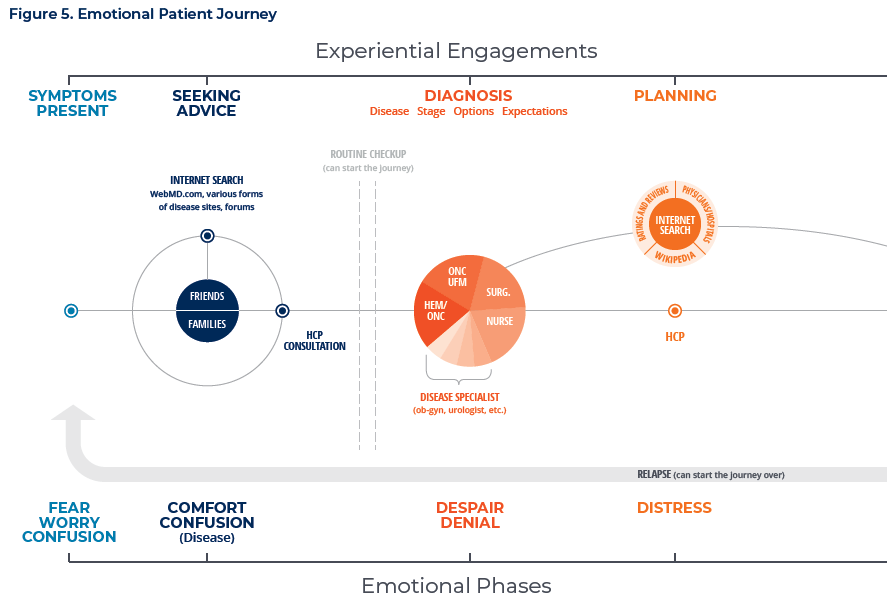
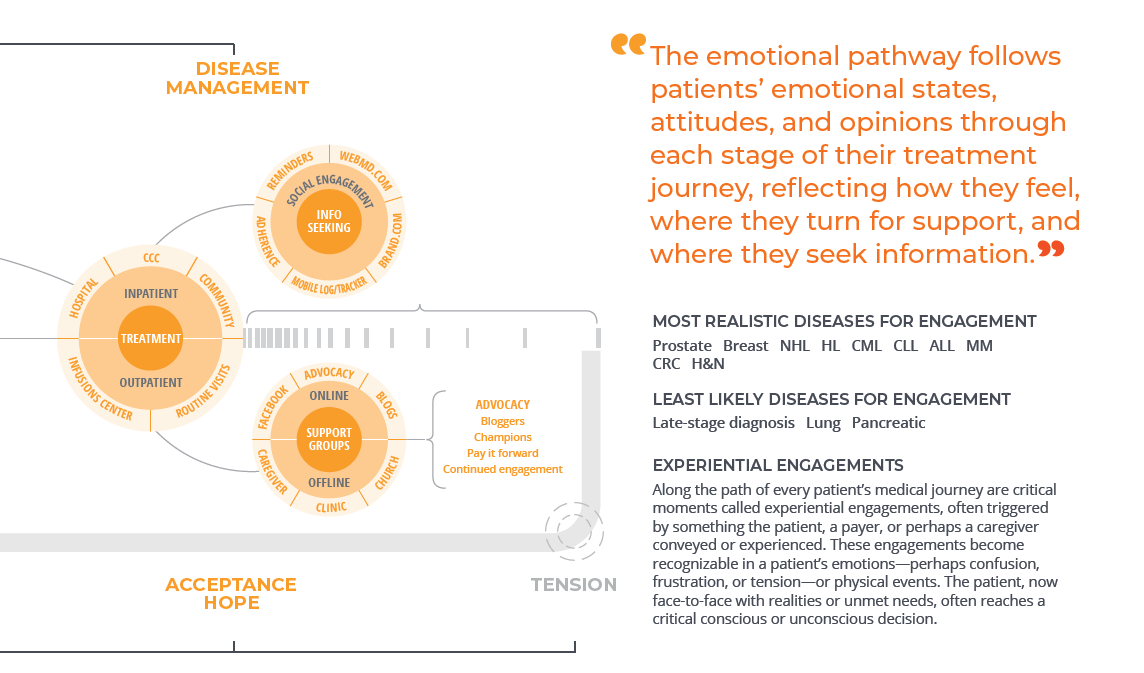
Fortunately, enrollment rates and study timelines can be vastly improved by understanding the patient pathway and working to meet patients where they are as they travel along it.