Introduction to SLE
Systemic lupus erythematosus (SLE) is an autoimmune disease that causes the immune system to produce several types of antibodies, particularly against cell nuclei. This disease is extremely heterogeneous in how it manifests, which leads to significant problems and delays in diagnosis. The condition most frequently affects the skin, joints and muscles, but can also disrupt other organs and systems, like the kidneys, heart, central nervous systems and others. The prevalence of lupus is approximately 50 patients per 100,000 in the United States. There are significant differences in the disease prevalence among different races. For example, Eastern Asians (excluding Japanese), African Americans and Hispanics are affected more frequently by the disease than other races. In addition, the prevalence of SLE is higher among women (up to nine times) than men.
History of Drug Development in SLE
Despite the disease prevalence, there is no effective treatment for SLE. Since the approval of aspirin in 1948, and then hydroxychloroquine and steroids in 1955, there has been only one drug — Belimumab, in 2011 — that was approved by FDA. Before and after Belimumab, a significant number of drugs have failed at different stages of development.
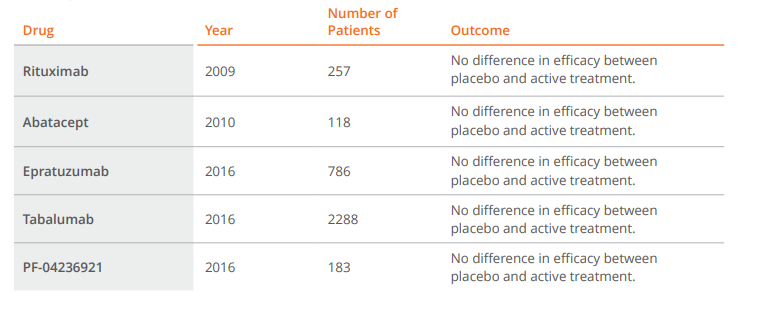
Drug development for SLE has suffered many setbacks, especially in the last few years.
Placebo Response Rate
Common issues that arise during SLE trials include high placebo response rates and the relatively small difference between active treatment and placebo arms. Even trials that met efficacy endpoints — such as Belimumab registration trials — still faced similar challenges. What this demonstrates is a multifaceted challenge, which all studies need to address in order to be successful.
Definition of Population
It starts with defining in protocol the patient population that should be enrolled in the trial. As mentioned earlier, SLE is a disease with very heterogeneous manifestations that make it difficult to diagnose. In addition, there is not a single test that can either confirm or exclude SLE, and there are several diagnosis criteria, which do not necessarily completely overlap with each other (ACR, SLICC). Serology tests (like anti-nuclear antibodies or anti-DNA) play a role in diagnosis, but they may become negative during the course of the disease. A requirement for positive ANA and anti-DNA will increase the probability of enrolled patients to actually have SLE (possibly increasing the difference between active treatment and placebo). This can lead to significant increases in the screening failure rate, thereby reducing the enrolment rate in an already difficult-to-enroll indication.
Disease activity at baseline in protocols is usually defined using two indices — Systemic Lupus Erythematosus Disease Index (SLEDAI) together with its many variations and British Isle Lupus Assessment (BILAG). Defining a higher SLEDAI score at baseline (or requiring more BILAG A or BILAG B scores) will result in patients with higher disease activity. It is easier to demonstrate decrease in disease activity in such patients. Such populations should have a lower placebo response rate (assuming other factors affecting placebo response rate are the same) than a group of patients with lower baseline disease activity. However, setting the required SLEDAI or BILAG at the higher level leads to more challenges in enrolment. Similar to serology requirements, a balance needs to be achieved to increase the probability of success, in both results and enrollment
Concomitant Medication
Patients with active SLE will have different therapies aimed at decreasing disease activities — steroids and immunosuppressants. However, reducing or washing out these therapies prior to the study is not feasible. Aside from ethical concerns, there would be an increased risk of patients experiencing disease flares, making them unsuitable for a clinical study. On the other hand, these therapies have the potential to affect efficacy outcomes, which will likely increase the placebo response rate. Steroids present another special challenge due to the frequency of their use, and because they are efficacious in this indication (their safety profile is the reason they are not considered to be a longterm solution). The majority of protocols mandate steroid tapering during the study (providing a patient’s clinical status allows it) to address the issue. This is not an easy process, though, as there is no standard guideline for steroid tapering and different physicians follow various protocols. In addition, they have different thresholds as well as different time points to start tapering steroids. All of these factors create challenges and affect outcomes of SLE trials.
Efficacy Endpoints
We already discussed different indices to measure disease activity at entry. The endpoints used in efficacy SLE trials are even more complex. There are mainly two types of endpoints — Systemic Lupus Erythematosus Responder Index (SRI-4 or SRI-5) and BILAG-Based Composite Lupus Assessment (BICLA). The first one is based more on the SLEDAI index, the second one more on BILAG.
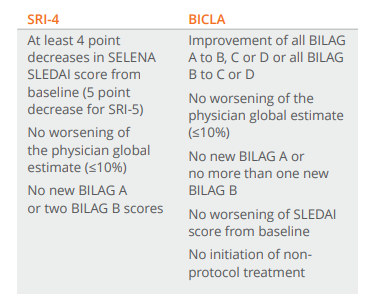
Both of these endpoints are highly subjective in nature. This translates into inter-rater variability and additional “noise” in the data, which cannot be fully eliminated. Placebo response rate and overall additional variability coming from this contributes to failures in many lupus studies.
One mitigation to the risks of incorrectly diagnosed patients being enrolled, and variability in endpoints assessments, is to implement an additional review of patients’ eligibility and of endpoints. This is done in different ways on SLE studies. The ideal, and also the most detailed process, requires a group of peers who are thoroughly familiar both with SLEDAI and BILAG scoring as well as lupus trials. Before being randomised, each patient is reviewed by this team and differences are discussed with investigators. The same process is applied to review each patient’s data for endpoint assessments. This review allows for increased consistency and the early identification of incorrectly enrolled patients, as well as possible needs for training.
Summary
SLE is probably one of the most challenging indications for drug development. Without understanding its challenges, as well as ways of addressing them, it is very hard to execute a successful trial, even with a drug that may be successful. It is also difficult to replicate Phase II results in larger trials, where the issues described above are enhanced. There are some promising drugs currently in different stages of development for SLE. Hopefully the lessons learned from past challenges will allow sponsors to successfully bring new therapies to the market.
