Synopsis
The percentage of oncology patients participating in clinical trials is remarkably low: 8.1 percent according to a recent meta-analysis. While this is more encouraging than the commonly cited value of 3 percent, it is nonetheless disappointingly low and explains the daunting recruitment challenges that sponsors face in most oncology trials.
Low participation rates are largely attributed to access issues (the availability of trials in the right geography for a given cancer type or stage) and eligibility restrictions. However, a number of other factors often compound the situation, including a heavy patient burden (in terms of clinic visits, tissue sampling requirements, etc.), patient misconceptions concerning trials, lack of awareness on the part of patients and physicians, and a failure to reach patients with study information at the right time in their treatment journey.
Cancer patients frequently rely on their physicians to inform them of trials for which they might be eligible. Meanwhile, many investigators appear to wait for the ideal study participants to walk through their door at just the right time in their treatment progression. As a result of these two factors, which ultimately leave a key aspect of patient recruitment to chance, it is little wonder that most trials experience delays due to slow enrollment.
Fortunately, enrollment rates and study timelines can be vastly improved by understanding the patient pathway and working to meet patients where they are as they travel along it.
How the Treatment Journey Impacts Site Identification and Patient Recruitment
The site identification process for all clinical trials should take into consideration the type of treatment center where patients who fit the target profile will present for diagnosis and treatment. It is, however, especially important to do so in oncology trials due to the complexities in treatment across tumor types and disease stages. Academic centers tend to treat patients with rare or advanced cancers, while community physicians tend to treat patients who are in first-line treatment for more common tumor types. Indeed, in the U.S., 85 percent of patients receive treatment at community facilities versus 15 percent in larger academic centers.
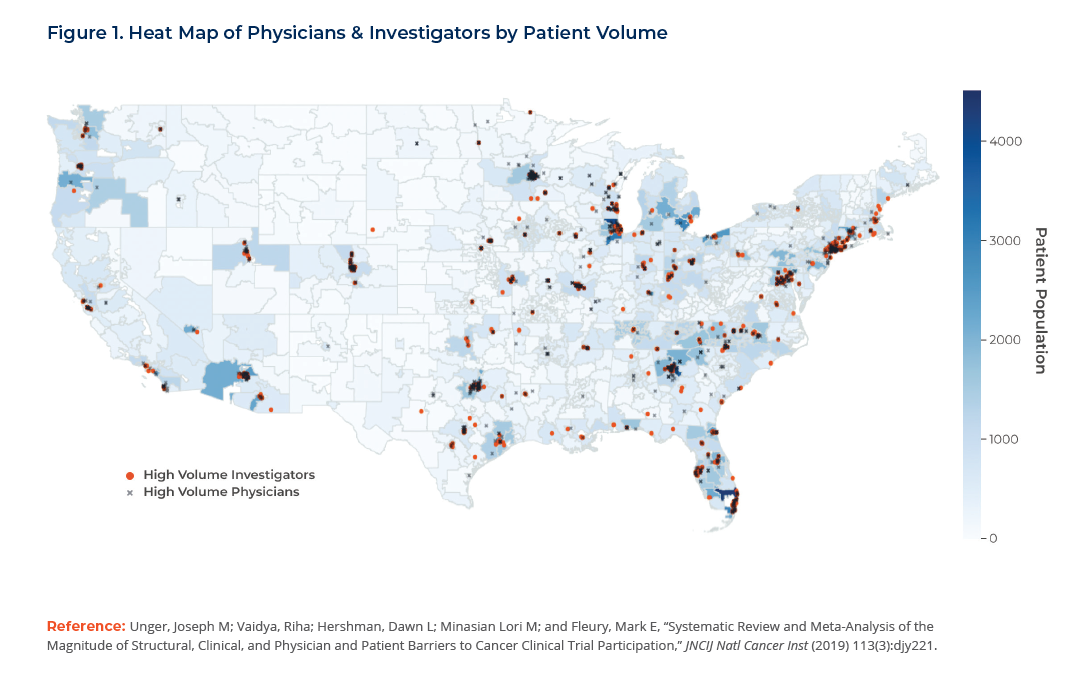
The process of identifying the best sites for a clinical trial is data-driven. Scores of databases are available to provide insight into the top prescribers by indication, and sophisticated algorithms can be applied to prioritize investigators based on any number of criteria including their experience, capabilities, facilities and performance history. The results can then be overlaid onto a map at a granular geographic level indicating where patients with a given diagnosis are physically located. To inform site selection, the results can be displayed as a “heat map” indicating the places of greatest overlap between qualified sites and high numbers of patients. (See Figure 1.)
Further, it is possible to analyze patterns in the treatment pathway for a given tumor type to reveal which medical specialties patients are visiting and to model the local and global referral process. (See Figures 2,3.)
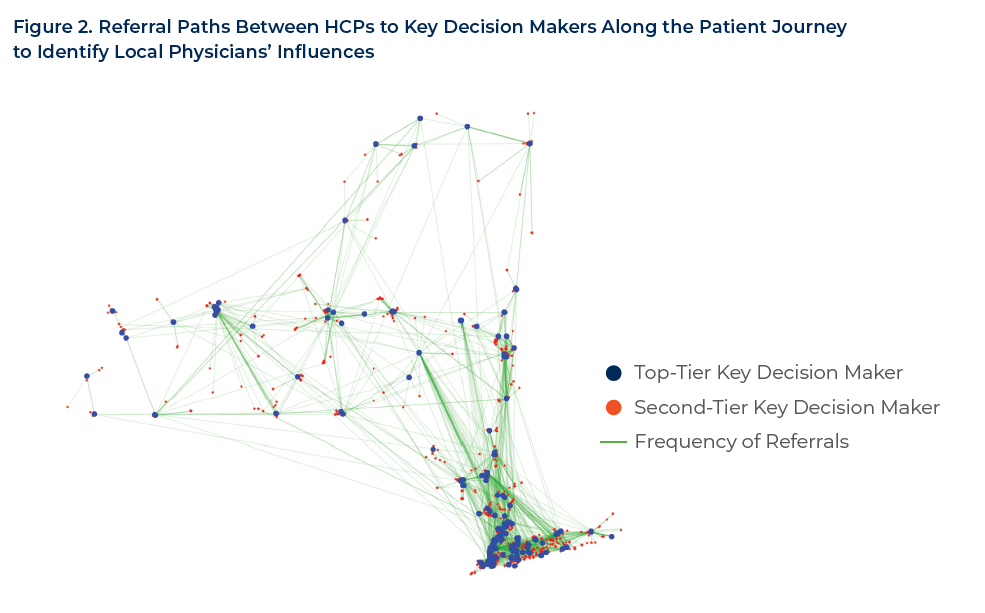
In this example, we identified top- and second-tier key decision makers (KDMs) among oncologists in New York state to promote a specific chemotherapy/immunotherapy drug. (Traditional approaches to KDM-mapping rely on signals available to everyone else, resulting in the same lists.) We mapped referrals from one physician to another as an indicator of recognized domain expertise and used referrals as a measure of influence. Using this approach, we were able to reveal and influence the right patient population by understanding the relationships between the numerous healthcare systems and patient facilities. The output showed the shared percentage of patient referral influence for the disease state spanning across the hospital setting, the community-based care establishments and digital engagement landscape.
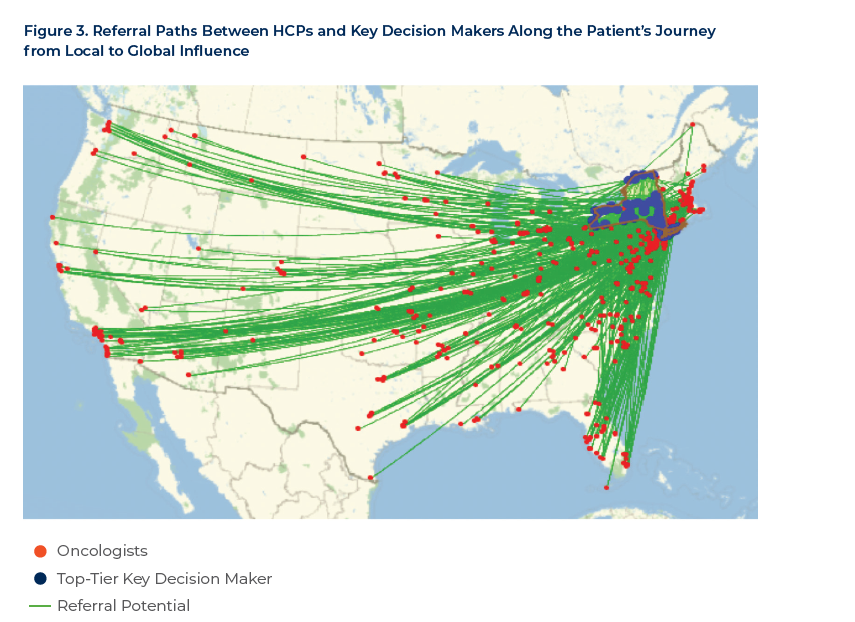
As seen in Figure 3, we then scaled geo-information up and down to the national or state level and cross-referenced it with patient volume and referral frequency. This included granular filters all the way down to the physician specialty and ZIP code level, resulting in a ranking of oncologists for each geographic area by a number of salient traits, cross-validated against an external source. The decile-ranked patient populations increased awareness and informed the true disease state prevalence mapped to the diagnosis to help better position the right audience, message and channel, geographically ranked for the trial.
Other mapping analyses that can be utilized include the following:
- Multidisciplinary treatment team composition – Detailing an oncology patients’ actual team of healthcare providers (HCPs) to optimize awareness campaigns
- Drivers of and barriers to referral behavior – Deploying targeted research to identify drivers important to and potential barriers for the investigators and referring healthcare providers
- Referrer channels and content – Mapping the right channels and content based on historical prevalence and preference
However, simply knowing where to target patients based on where they get treatment is not sufficient to forge an adequate site selection and recruitment strategy. It is often necessary to make a basic decision: should sites that are already seeing patients be activated? Or, is it preferable— even necessary—to activate other sites that may not yet be seeing patients, but that may be more capable of handling the complexity and rigors of the given protocol and that have all of the auxiliary services and resources? In other words, is it preferable to “go where the patients are” because of their progression through the treatment journey, or to “drive patients to where you want them to be,” in effect disrupting the patient journey?
The decision to work with sites where patients are not naturally presenting requires a different recruitment strategy—one that makes strong use of referral networks and supplies referring sites with the information they need both for themselves and for their patients. In this way, the site identification strategy and the patient recruitment and engagement strategy are intertwined and informed by the patient journey.
Selecting and Priming Sites
Patient recruitment will naturally be more efficient if sponsors (or their contract research organization (CRO) delegates) perform proper due diligence into the type and number of patients that potential sites treat. While this is a standard practice as part of the feasibility and site identification process, it may not always explore the patient profile and protocol requirements in enough detail to be fully effective. The process should:
- Ensure that sites truly understand the target patient profile. This demands a focus on the key points that investigators should understand about patient eligibility, to the point of being extremely specific about what they should be searching for in their patient charts and practice database. This may mean probing for the answers that are needed, rather than settling for the answers that one wants to hear.
- Entice sites to participate while explaining clearly what will actually be required. Certainly, a by-product of discussions with sites at this stage is to engender their interest in participation, but that cannot be done at the expense of being forthright about what kind of patients will be sought and what type of capabilities will be required.
- Prime each site to consider the most challenging aspects of recruitment in detail. For example, many oncology protocols are looking for patients with specific genetic mutations. When that is the case, will the sponsor provide testing centrally to determine patient eligibility, or are sites expected to already know the patient’s mutation status? If the latter, sites must be asked if they routinely perform the testing themselves of if they have easy local access to a method of testing that will be both acceptable and reimbursed.
- Verify the patient journey. Sponsors need to consider where prospective patients will be in their treatment journey at the point of protocol enrollment. Understanding this will help to determine if a given site will serve as a natural intersection point for patients, prior to selection of other treatment options. Gathering this insight might entail adding two or three additional questions to the feasibility questionnaire. While sponsors are often reluctant to overload the feasibility effort and make it more cumbersome for sites, being able to probe on these points undoubtedly yields benefits “down the road.”
- Be revisited as needed as the protocol changes. Often, initial input from sites is gathered before the protocol is finalized, and changes to the protocol can impact sites’ ability to carry out the protocol and/or to recruit patients. Initial feasibility data may need to be validated following significant protocol changes. However, the appropriate balance should be struck between not wanting to burden sites with every minor protocol change and waiting too long to discover that a given change will have a significant impact, such as eliminating an entire country or specific sites from trial participation.
- Ensure that information is carried forward as the process progresses through site activation. All those in contact with the site, from the initial discussions onwards must share information and lessons learned, adding to the body of knowledge about the site. This supports optimum efficiency and provides the best experience for sites.
- Verify information at the pre-study visit. The authenticity of information previously collected should be verified. The Clinical Research Associate (CRA) should ask questions such as: have you looked through your database to confirm your patient counts, or are we working with estimates? Can we look through some charts to verify that you are, in fact, seeing three patients a month with this mutation?
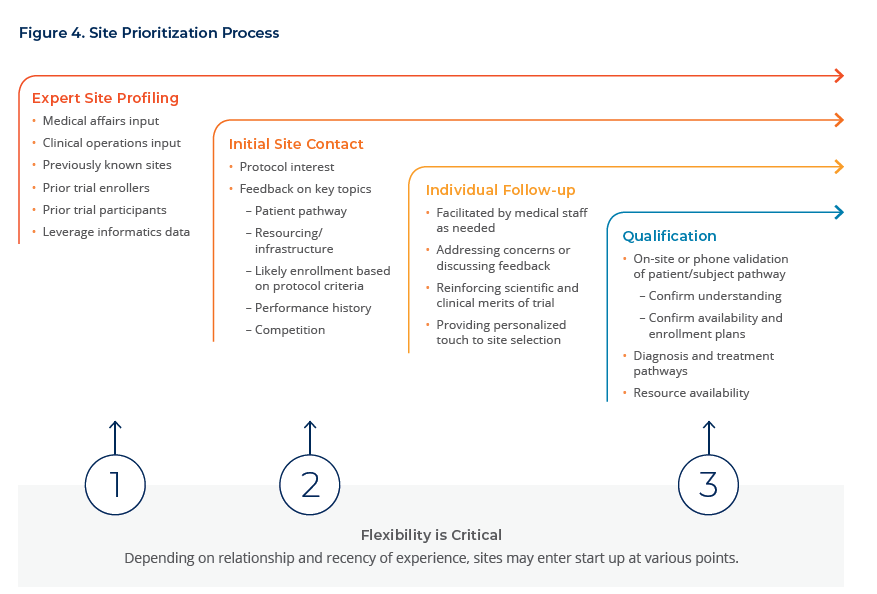
Figure 4 illustrates a thorough site selection process that combines data, past experience, and careful vetting to identify sites that are qualified and have access to patients at the right stage of their diagnosis and treatment pathway.
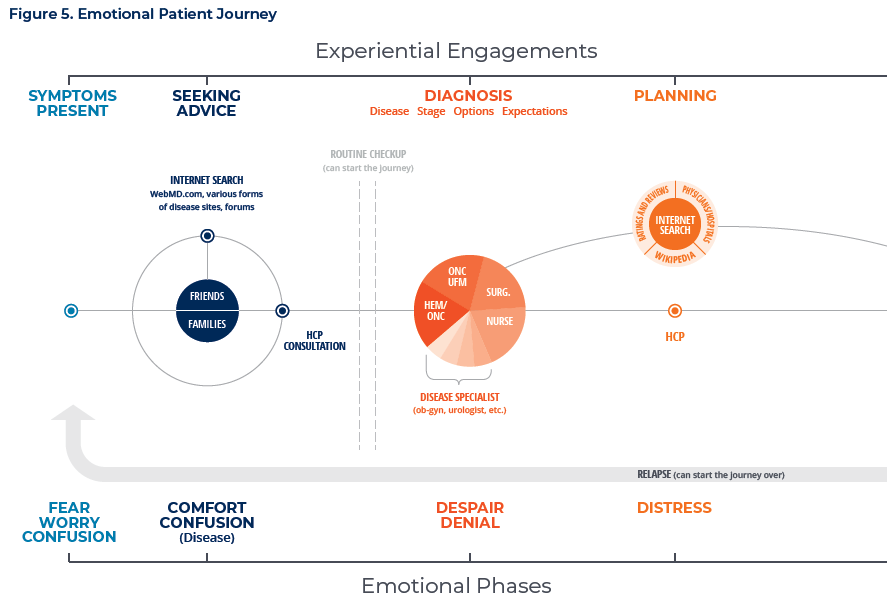
Understanding the Influence of the Emotional Pathway
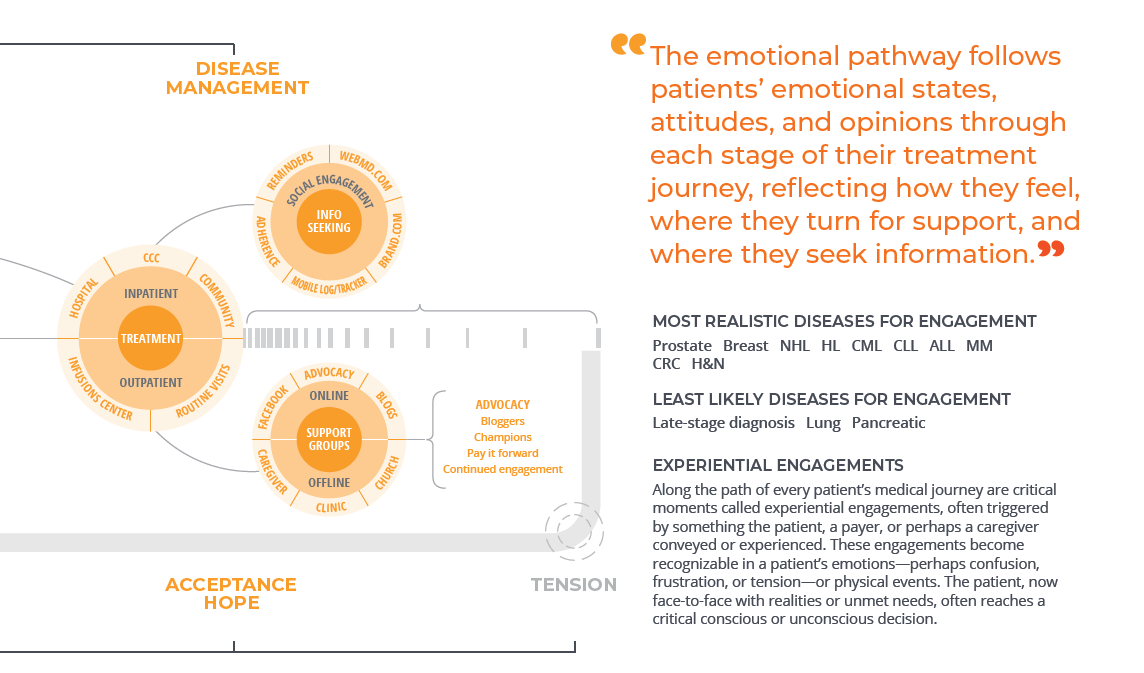
Finding patients at the right point in the treatment pathway is not the only challenge; as patients experience cancer, they traverse both a treatment pathway and an emotional pathway. The treatment journey describes the course of the disease from diagnosis, through treatment to remission, cure or mortality. The emotional pathway, on the other hand, follows patients’ emotional states, attitudes and opinions through each stage of their treatment journey. It reflects how they feel, where they turn for support, and where they seek information. Figure 5 illustrates the typical emotional journey for oncology patients at key points along the treatment pathway.
Although the practice of using hard data to make decisions is continuous throughout the recruitment process, developing an understanding of the emotional pathway and the patient perspective layers in a more personal sensibility. This is especially critical to patient recruitment in oncology because of the range of experiences that people have with the disease and the uniqueness of each patient’s ability to cope both physically and mentally—nuances that should be appreciated when presenting clinical trials as a viable option for patients.
Insights into the emotional pathway for a given type of cancer are developed by a variety of means: social listening, interviews with key opinion leaders (KOLs), talking to primary care physicians and specialists, and discussions with patient advocacy groups. Social listening, in particular, can be very valuable in that it provides an opportunity to be privy to unfiltered, authentic conversations of both patients and caregivers. One can identify, for example, where patients go to discuss their condition and seek counsel from others, how they describe their emotional state, what challenges they’re facing, what they’re concerned about, how they’re reacting to treatment regimens, and so forth.
Such careful listening can lead to the discovery of robust audience insights that can drive the recruitment strategy. For example, if a protocol is seeking breast cancer patients who have failed first-line therapy and whose tumor has metastasized, recruitment efforts should recognize that those patients have progressed to another phase in their emotional journey. Those women who are younger may be concerned about spending quality time with their children and extended family, rather than continuing further treatment. Having ridden the waves of hope in the belief that they could be cured, they are now faced with the prospect that a clinical trial might be one of their few remaining options. Sites will be having conversations with these patients knowing that their emotional strength will be very low and that their extended family may have a strong voice in any decisions regarding participation in a clinical trial. In this instance, targeting media ads toward family members, as well as having information about study participation for families to read and understand, will help them in making that decision.
Reaching Patients at the Right Points in Their Journey
An understanding of the patient journey—meaning both the treatment and emotional pathways—can be used to develop the media strategy and messaging platform that will help sites find the right patients for the study. Recruitment communications can either be via a centralized campaign or via site-specific recruitment plans.
Whereas the treatment journey describes the typical course of the disease and treatment paradigm for a patient, the emotional pathway encompasses patient and caregiver needs, preferences, and characteristics that help shape the channel strategy and messaging. When the patient voice is reflected in copy and images, communications are more engaging and resonate with the patients and/or caregivers.
Headline
Factors Influencing Patient Outreach Strategies
- Prevalence of tumor type
- Stage of cancer
- Aggressiveness of cancer
- Role of caregivers
- Where patients/caregivers seek information and support
- Sphere of influence
Tactical Elements
- Decision-support materials for referring physicians. If patients will likely be referred to sites by other physicians, it is important to provide decision-support materials to those referring physicians so that they can discuss the trial as a potential option for patients and conduct appropriate pre-screening to determine eligibility. Ultimately, this approach reduces the burden on sites.
- Patient materials for investigators. Especially in oncology, patients usually do not consent to participate right away. Rather, the informed consent process requires a thoughtful discussion between the patient, the caregiver, the investigator and often the referring oncologist. Thus, it is helpful to provide investigators with materials that they can use to support this discussion. Often, visual aids are good resources for conveying information to patients in these pre-enrollment discussions, and research into the patient pathway can inform the development of these aids. Another option is to provide an information-rich website to which the investigator can direct referring oncologists, patients and caregivers.
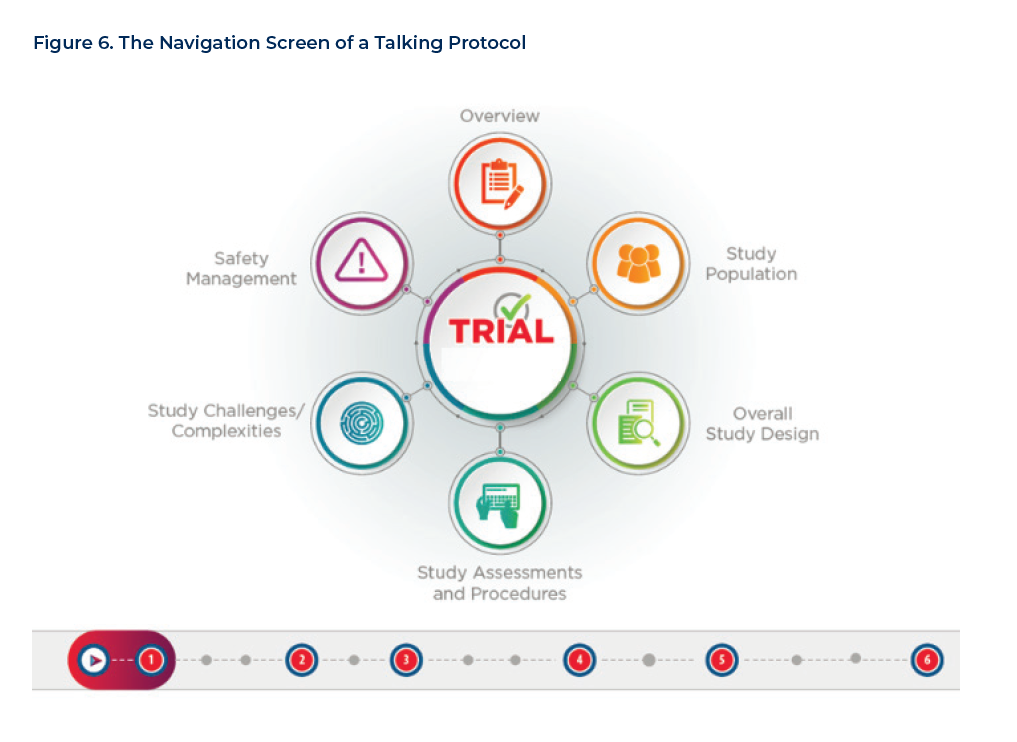
- Talking Trial Protocols. These multimedia, interactive presentations of study-related information give users the ability to self-navigate through their training for higher engagement. Users (study staff, investigators and enrolled patients) can click on any section of the trial protocol of interest, in the order that they want. Figure 6 illustrates the navigation options of a typical talking protocol. The elements might include data presented graphically, written stakeholder insights, video testimonials, etc., and access can be provided via a password-protected mobile app. Analytics and survey questions can capture valuable data on which aspects of protocol are most engaging, hardest to understand, or of greatest importance to the user.
- Digital Awareness Programs. In oncology, folding digital into the comprehensive enrollment program is not typical. Typically a study website is not even developed, which further enhances the importance of sites’ efforts being optimized towards the most efficient processes. Historically, online platforms are utilized to drive study awareness, and direct interested patients toward study sites. Often a mix of digital and social platforms are deployed. Common tools include Facebook advertising, Google search and Google Audience Network (display). Digital awareness and engagement campaigns are an increasingly-important component of a comprehensive oncology enrollment strategy.
Both the treatment and emotional pathways inform the selection of tactical elements created for a trial and used by a site. For example, if a trial is targeting first-line patients predominantly seen in the community, but the trial is being driven to large academic and research centers due to procedural complexity, then decision-support materials for referrers and online awareness programs can be used to connect the patient’s treatment pathway with the site. Online awareness programs can be effective both with very common and with very rare cancers, depending on how the population is targeted and where the sites are located. Once patients are at the trial site, patient materials become critical for engaging them in their emotional journey and connecting them to the trial protocol.
Conclusion
By understanding the patient journey—both the treatment and emotional pathway that patients travel over the course of their disease—sponsors can better identify appropriate sites for clinical trials and develop targeted patient recruitment strategies. They can avoid waiting for patients to arrive by chance at sites and at the right point in their journey for a given trial, as well as disrupting the patient journey to get patients where they need to be.
