In the high-stakes pharmaceutical arena, cooperation among manufacturers of competing brands is something of an unusual concept. With the rise of single shared system Risk Evaluation and Mitigation Strategy (REMS) requirements, however, pharmaceutical companies are faced with the need to coordinate and reach consensus with their rivals in order to effectively meet the demands of the FDA.
A REMS is an FDA-mandated requirement placed on products that are approvd but that need some additional action to ensure the benefits of the product outweigh the risks. The majority of REMS affect individual companies.
Single shared system REMS (SSSRs), meanwhile, are a growing trend in which the FDA can require competing companies to collaborate on a REMS program for marketed products that are the same or similar. The FDA has mandated that a drug that is the subject of an abbreviated new drug application (ANDA) and the reference listed drug shall use a single, shared system; to reduce the burden to the healthcare system of having multiple REMS for multiple products in the same class, the FDA has also encouraged SSSRs that involve multiple innovators. SSSRs include more than one sponsor, who must share Elements to Assure Safe Use (ETASU), databases and infrastructure; a single REMS document, REMS materials and supporting documents; and most or all components of the REMS Assessment. ETASU can include call centers or websites for delivering information to physicians and patients, patient registries and/or education for prescribers.
Participants in SSSR may face difficulties in communicating, dividing responsibilities and costs, trusting each other and generally coming to agreement in a timely manner to meet deadlines and goals. As a result of these challenges, these companies run the risk of negotiating REMS commitments with the FDA that they are unable to fulfill or that are unduly burdensome, ultimately threatening the standing of their brand in the market.
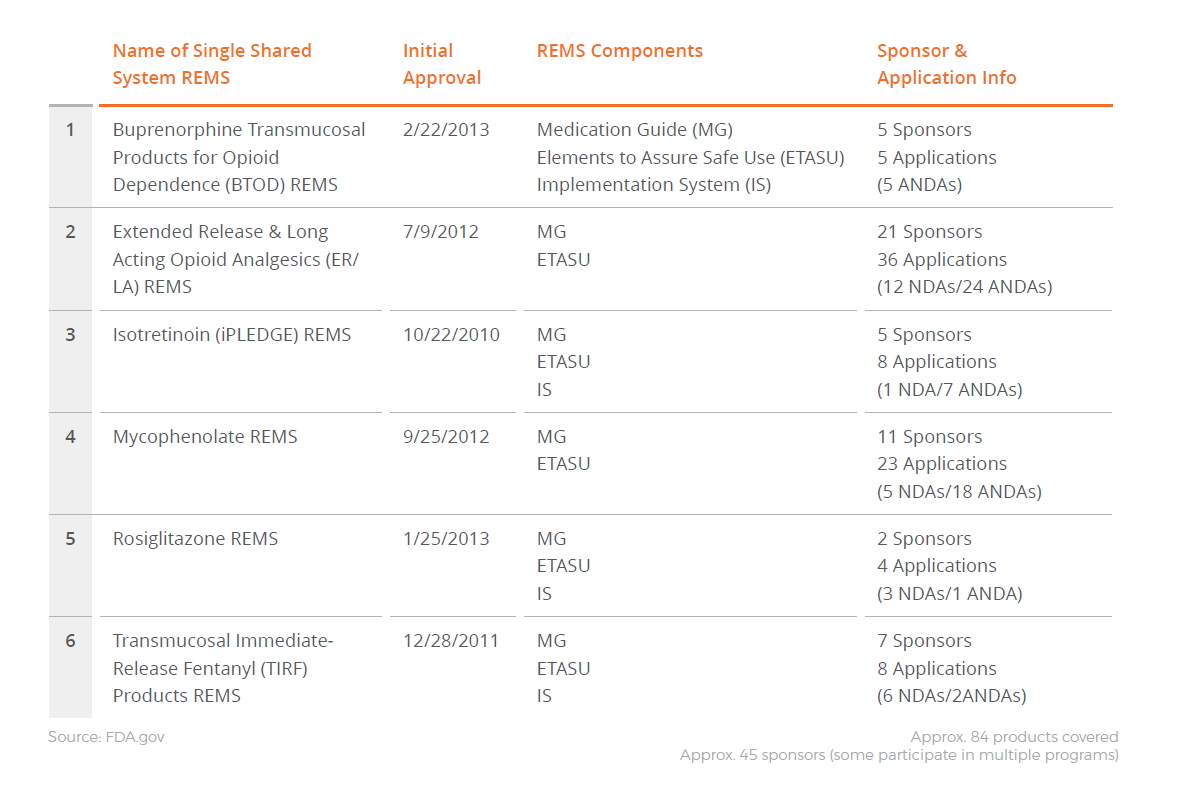
At the time of this writing, six single shared system REMS are currently approved (Figure 1), involving approximately 84 products and 45 sponsors, some of whom participate in multiple programs. The number of sponsors involved in any individual SSSR ranges from two to just over 20. The number of SSSR programs is only expected to increase as individual products with REMS with ETASU face loss of exclusivity (LOE) and generic entry.
This article will focus on the timelines—and the key challenges that can impact those timelines—in each of four main “phases” associated with the implementation of SSSR programs. By understanding the core challenges and complexities involved in collaboratively implementing an SSSR, companies may be better positioned to create and execute a successful and compliant REMS program.
Figure 1: Existing Single Shared System REMS
The Four Phases
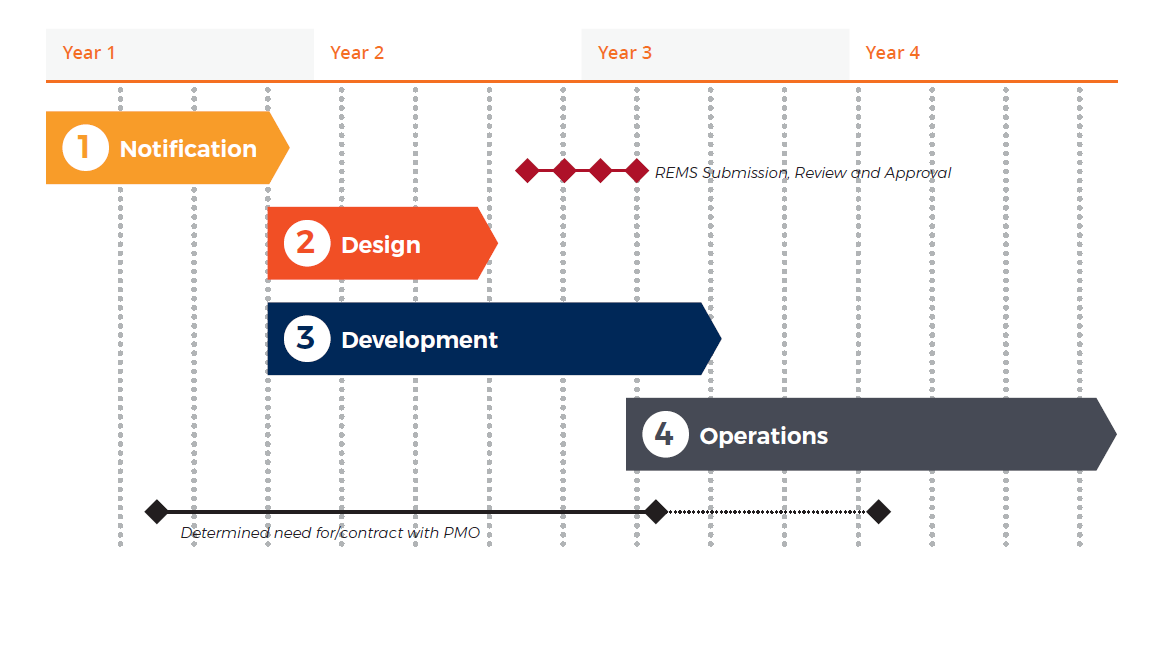
Before we take a look at each phase independently, it is important to align on the general definitions and timelines associated with the design, development and implementation of an SSSR program (Figure 2).
The Notification phase begins the moment the FDA issues a letter to the sponsors letting them know they need to work together to develop a shared system program. The Design phase is the period during which the sponsors collaborate to write the REMS submission for the agency, which includes the public-facing REMS document, the confidential REMS supporting document and all the associated materials. The Development phase typically runs in parallel with the Design phase and involves the building of the components that will support the REMS once it is approved. Finally, the Operations phase is the ongoing management and maintenance of the program after it goes live.
Figure 2: General Timelines
Phase One | Notification
Phase one can take anywhere from six months to three years to complete.* Typically, though, most sponsor teams tend to complete this phase in around 12 months. The phase begins when the REMS letter is issued by the FDA and received by the sponsors. The initial task for the sponsors upon receiving the letter is to connect and talk to each other, which is not necessarily as straightforward as it sounds. They will first need to determine whether or not there is a need to retain any form of external counsel, whether it be general counsel, antitrust counsel, or both.
Next, the sponsor collective must develop an agreement—often called either a Memorandum of Understanding (MOU) or a REMS Participant Agreement (RPA)—that outlines how they are going to work together to execute the program. This document typically includes such issues as high-level governance, cost sharing, decisionmaking process, and entry and exit processes for new participants or exiting participants. Each of the sponsors needs to sign this core document so that they are all working under a common set of rules when they move forward. Developing the document can take a significant amount of time depending on the number of sponsors involved, familiarity of sponsors with shared REMS programs and availability of dedicated counsel.
The remaining task in phase one is to determine how to manage the overall program. The sponsors can choose to collectively run the program or hire a third party to help manage it. A Program Management Office (PMO) can serve as a neutral third party designed to facilitate the myriad legal, financial and operational challenges of initiating and implementing an SSSR. A wide variety of PMO structures, roles, and responsibilities exist (see sidebar for more details).
The first phase of a shared REMS program can be the most challenging phase, especially for sponsors with limited shared REMS experience. Simply collaborating with competitors is the first hurdle and is more complicated when branded and generic organizations are involved in legal action. Whenever competitors in the marketplace are asked to work together, there will likely be antitrust and competitive confidentiality issues that will need to be addressed from a legal perspective.
Headline
Core Challenges/Impact Factors in Phase One
- Collaborating with competitors, especially where branded and generic organizations may be involved in legal action
- Retaining antitrust external counsel
- Developing a Memorandum of Understanding (MOU) or a REMS Participant Agreement (RPA)
- Deciding on a PMO model: may begin in phase one and continue into phase two or may come up in later phases
Phase Two | REMS Design
Phase two does not typically begin until an MOU has been fully executed unless one sponsor begins or has begun work independently of the group. Whether on their own or with the help of a vendor, the sponsors must develop the draft REMS documents, which typically takes three to six months. Once the REMS and the REMS supporting documents are developed, the submission process can begin with the FDA. Once the FDA determines the REMS is in an approvable format, the sponsors submit a final version, and the FDA will formally issue its approval.
The challenges in phase two are predominantly associated with sponsor choice of vendor model and the complexity of the program under consideration. The sponsors must gain consensus on the framework they want to use to write the REMS. If it is a branded product that already had a REMS in place, there may be a push to work from the existing program and adapt it to accommodate multiple products.
Understanding the complexity of the requirements for the program is another challenge. Some REMS can be straightforward, simply calling for an informational website and a call center for physicians or patients who have questions. However, if the REMS calls for any kind of restricted distribution or a registry to be put in place, the REMS becomes more complex. The number and type of ETASU can also impact the complexity of the program, and more complex programs take more time to gain agreement on and write.
The complexity of the program will also likely impact the review timelines and negotiations with the FDA. The review process can take as little as four or five months, or it can take years if there is a lot of back and forth about how best to build the program.
PMO Models and Responsibilities
While PMOs vary from one program to another, the following provides an overview of the typical structures, roles and responsibilities.
Types of PMO models
- Independent: A neutral, third-party organization is hired to serve as PMO and does not provide any REMS services beyond program management responsibilities
- Prime: A neutral organization is hired to serve as PMO and may also provide other REMS services (e.g., call center or help desk)
- Sponsor managed: No third party is hired; sponsor organizations provide program management personnel
Typical PMO Responsibilities
- Program/sponsor management: Manage day-to-day operations of the program, including project plan, sponsor meetings and document management
- Vendor management: Support procurement and management of vendors that provide REMS services
- Finance/budget management: Establish and manage budget for program and support allocation of costs among sponsors
- Optional: PMO contracts directly with vendors and manages program invoicing (versus sponsors contracting individually with vendors)
Headline
Core Challenges/Impact Factors in Phase Two
- Gaining consensus on the framework for the REMS: e.g., working from an approved REMS versus developing a program from scratch
- Deciding whether to use a third party vendor to write the REMS
- Understanding the complexity of the program requirements needed to ensure patient safety • Adjusting to review times and potential need for design negotiations with FDA
Phase Three | REMS Development
The third phase typically begins in parallel with phase two to enable vendor selection and contracting to occur for the building of websites, staffing of call centers and creation of patient registries. This is important because once the FDA approves the REMS, the agency will want the program up and running as soon as possible, typically within 30 to 60 days. It would be impossible to evaluate, select and contract vendors and get them to build and validate all of the components that need to be ready to execute the program in that narrow window. Therefore, the development of the program mechanics must occur in parallel—and to some extent at risk—as the program is designed.
Once selected vendors are under contract, they need to begin developing the program elements based on the current design of the REMS, knowing that at some point after the initial FDA submission, the program design may need to change. Sponsor companies should work collaboratively with the agency to set expectations for the program and come to a common set of assumptions in order to reduce development risk as much as possible.
The challenges in phase three are predominantly associated with program design and the number/ type of ETASU requiring independent vendors and the associated timelines for RFP processes, vendor selection and contracting. The type of PMO model being used is also an issue, as the PMO will need to be on board before it can contract with other vendors.
The number of sponsors and their familiarity with developing SSSR programs is another issue at this stage. The more opinions added to the mix, the longer it can take to come to a consensus and make a decision. Even with the best of intentions, issues that may take one company four weeks to resolve may take six companies collectively four months to resolve.
Headline
Core Challenges/Impact Factors in Phase Three
- Number and complexity of ETASU requiring independent vendors— timelines for RFP process, vendor selection and contracting
- Type of PMO model being used (if any) and status of PMO onboarding
- Number of sponsors and familiarity with developing shared system programs • Working “at risk” ahead of program design approval
Phase Four | REMS Operations
Phase four begins once FDA approval of the REMS program has been obtained and the program goes live. This phase continues indefinitely. Once the program goes live, it remains so until the FDA deems it is no longer needed because the risk is sufficiently managed. Ongoing activities in phase four include (but are not limited to):
- Vendor management
- REMS modifications • Entry/exit of sponsors to and from the program
- Identification, evaluation, selection, contracting with additional vendors (for assessment report metrics, e.g., prescriber surveys, data collection)
During this period of time, a number of activities have to take place. For example, a communication plan might be needed to notify stakeholders that a new shared program is underway. Meanwhile, under the REMS, regular assessment reports must be developed.
Challenges in phase four are predominantly associated with management of and modifications to an approved program. A significant challenge is the ability of the program to meet the goals of the REMS. It may come to light that the goals that were put in place were not realistic. While the sponsors will do their best to meet those goals, if the goals are not being met over time, it may be necessary to have conversations about why they are not and whether modifications should be made to the program. The FDA itself may mandate modifications if the assessments reveal areas within the program that are not optimal.
An additional challenge as the REMS program proceeds is that turnover will likely occur within the sponsor group. New sponsors will have newly approved NDAs or ANDAs that fall under the REMS and will need to join, while other companies may cease marketing a product and choose to exit the program. Each situation has specific requirements in terms of what needs to take place to become a participant or to exit the program and complete the financial obligations.
One other challenge in the Operations phase is generally responding to FDA requests. The requested turnaround time for responses can sometimes be quite narrow, and when a large number of sponsors are involved, pulling together an agreed-upon response in a short amount of time can be difficult if not impossible. While the sponsors always do their best to respond in the timeline requested, they must be careful to manage expectations and communicate clearly with the FDA when a timely response is not possible.
Headline
Core Challenges/Impact Factors in Phase Four
- Ability of program to meet goals as defined in the REMS
- REMS modifications • Version control between FDA and sponsors
- Entry and exit of sponsors to the program—when is appropriate (pending or approved application status)
- Responding to FDA inquiries—turnaround time
Conclusion
SSSR programs are a growing trend, and there are few established models to follow. The FDA and the sponsor companies alike are still trying to figure out the optimal way of putting these programs together and managing them on an ongoing basis. While the challenges are numerous, they are not insurmountable. Simply understanding what the challenges are and what is required can put sponsors in a far better position to navigate them.
In an environment of competitors working together to accomplish the shared goals of a REMS, communication is key. Decisions need to be conducted such that all voices are heard. All sponsors must feel that they have an equal voice and access to program information in order to build the trust required to collaborate effectively. In this way, participants in single shared system REMS can overcome the challenges of working cooperatively with their competitors to meet the requirements of the FDA and ensure the safe use and adoption of their brands.
While only a few SSSR programs exist today, the industry can likely expect to see substantially more in the future, and they are affecting many different organizations as well as the FDA. Perhaps the rise in single shared system REMS will lead to a more standardized model to mitigate some of the challenges currently being seen.
Simply understanding what the challenges are and what is required can put sponsors in a far better position to navigate them.
Headline
Results
It’s a pretty simple word that’s used a lot in the business world, but what does it really mean?
When you cut through all the clutter, “results” means performing beyond expectations, eradicating challenges and achieving your business goals. It means not just dreaming it. But actually doing it.
Syneos Health Consulting is purpose-built to help biopharmaceutical and medical technology companies achieve results. Whether it’s seizing the leadership position in a new market, solving seemingly impossible challenges, or developing innovative approaches for success, we don’t quit until the desired results are delivered.
We offer the insight to help leaders develop powerful strategies, as well as the knowledge to ensure they’ll work in the real world. And as part of Syneos Health, we bring the global implementation capabilities needed to put even the most ambitious plans into action.
Contact
For more information on best practices in designing, developing and operationalizing single shared system REMS programs or Syneos Health Consulting’s capabilities to provide PMO services, please contact:
Jemma Contreras
Managing Director - Practice Area Lead
Risk & Program Management
Syneos Health Consulting
[email protected]
