ご案内
The problem of non-adherence to medications, especially for chronic conditions, is widely recognized as one of the most confounding and intractable obstacles to improving patient outcomes and reducing healthcare costs.
- According to the World HealthOrganization, medication adherence canhave a more direct impact on patientoutcomes than the treatment itself.1
- Nearly $300 billion is lost in additionalavoidable medical spending eachyear when patients don’t take theirmedicines as prescribed.2
Another important, often unrecognized, aspect to non-adherence is that it may lead prescribers to doubt the efficacy of medicines when they don’t obtain the outcomes seen in clinical trials.
- Nonadherence can account for up to 50 percent of treatment failures, approximately 125,000 deaths and up to 25 percent of hospitalizations each year in the United States.
Current methods of improving medication adherence for chronic health problems are mostly complex and have not yet been shown to be widely effective, making the full benefits of therapy difficult to demonstrate in realworld clinical practice. When all is said and done, a pharmaceutical company may spend twice as much getting the patient to the retail pharmacy counter as it spent on inventing and testing the drug to begin with. But then what happens?
- As many as 30 percent of people don’t pick up their prescribed medications.
- Among those who do pick up that first prescription, as many as 30 percent stop taking their medicine within 30 days.
- Up to 60 percent stop taking their medicine within six months.6,7
Focus on interventions to address thisn problem has intensified in recent years, however, aided by advances in technology that have opened up new channels for reinforcing adherence behaviors. In addition, quality-ofcare models are forcing change, evolving to be more patient-centric and outcomes-focused, with improving adherence a top priority.
For our second annual Patient Influence Adherence Report, Syneos Health™ set out to understand the factors currently influencing patient adherence behaviors at the retail pharmacy level and compare this with prior years’ data to understand adherence trends over time.
Methodology
For the third year in a row, we leveraged data from Adheris Health, a provider of dynamic patient performance programs that activate patients, improve outcomes and elevate brand performance. Adheris Health has one of the nation’s largest comprehensive networks for patient and prescriber access, with insight into 2.24 billion prescriptions each year, 35 pharmacy chains, over 29,900 pharmacies and 194 million people. For this report, we looked at the top 100 most prescribed retail pharmacy branded drugs for chronic conditions across 20 different therapeutic categories, and we followed over 200,000 “new-to-the-brand” patients—patients who filled a brand for the first time in the first quarter of 2017.
We collected a range of demographic data that outline key characteristics of the retail pharmacy patients (Fig. 1). Then we followed these new-to-the-brand patients over the next nine months in 2017 (Fig. 2).

We assessed their prescription utilization (refill behavior) against more than 30 product, patient, prescriber and payer variables to understand the most influential factors driving patient adherence or non-adherence, as measured by average patient days on therapy (PDOT or compliance)—that is, the number of days during the nine-month period when the patient had the prescription medication on hand. As this is the third year, we then took the data from all three years to understand how these factors have trended over time.
Key Findings
Slow but sure improvement
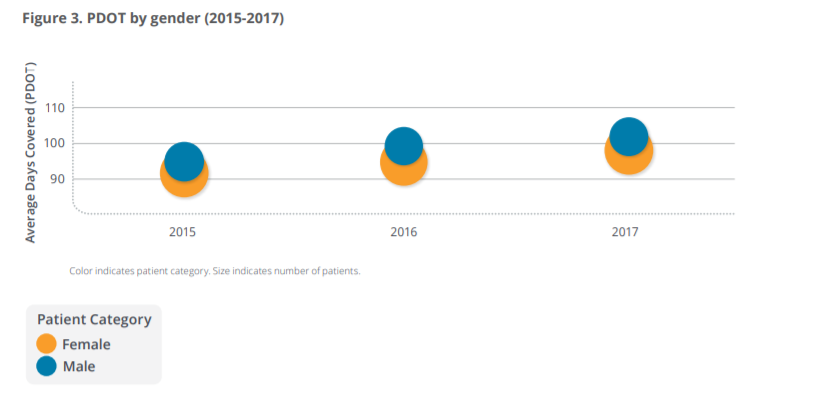
Patient adherence for new-to-the-brand patients, as measured by patient days on therapy (PDOT), has increased over the three years (2015-2017) we have been collecting this data. Average PDOT climbed from 92.8 in 2015, to 94.1 in 2016, and again up to 99.5 in 2017 (Fig. 3). In addition, the adherence trend line improved for both men and women. We continued to see that a gender gap in PDOT persists, although the gap narrowed somewhat in 2017.
The overall average improvement (5.7 percent from 2016 to 2017) is encouraging, as is the upward trend in PDOT for chronic conditions. Digital patient engagement tools; mobile health tracking technologies; healthcare IT (e.g., electronic medical records, e-prescribing); better coordinated, patient-centered care; and healthcare industry involvement and collaboration (including payers) are among the adherence strategies increasingly taking aim at the medication adherence challenge and, overall, may be having some impact.
Some therapeutic categories still lag behind
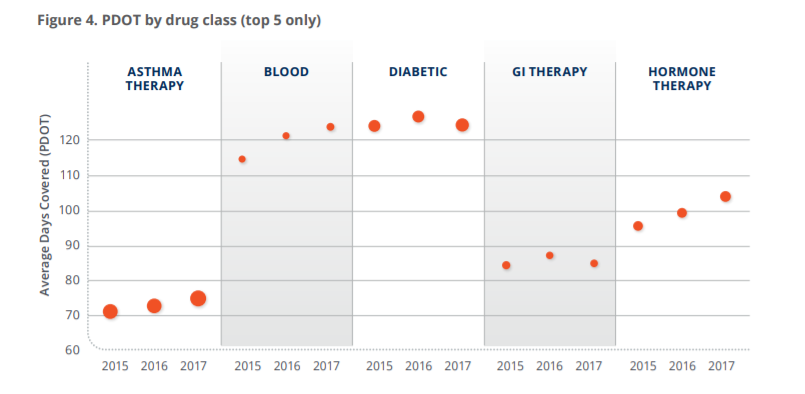
Although our data shows average PDOT trending upward over the last three years overall, there were differences in the trend line by therapeutic category (Fig. 4). The categories showing a generally upward trend from 2015 to 2017 were hormone therapies, blood thinners, ophthalmic and asthma therapies. Diabetes and GI therapies showed slight decreases from 2016 to 2017. While asthma PDOT increased from 2015 to 2017, this category still has a significantly lower compliant patient population by PDOT than the others in the top five largest therapeutic categories (by patient volume).
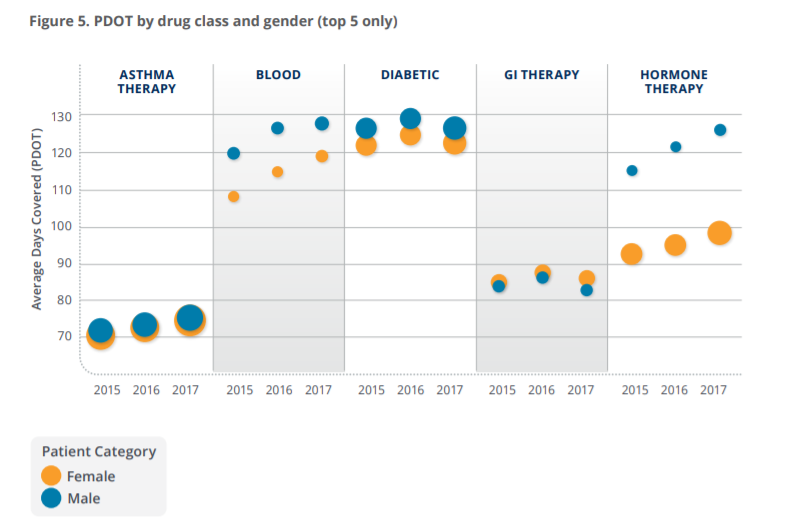
When we looked at adherence within individual categories, we again noted some gender differences (Fig. 5). In the asthma category, PDOT rates for men and women have climbed similarly over time; in 2017 they were virtually the same (74.9 and 74.2, respectively). In contrast, PDOT rates for men and women in the diabetes category trended similarly but PDOT was consistently higher for men than for women each year, with rates of 126.0 vs. 121.9, respectively, in 2017.
Certain prescribing specialties outperform others
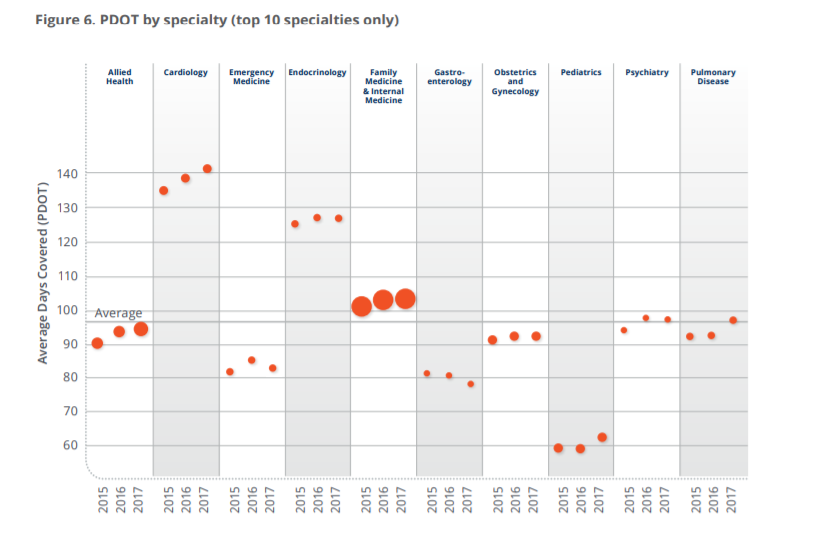
Across all prescribing specialties, the average PDOT in 2017 was 99.5. Three specialties outperformed this average; cardiology had the highest PDOT (141.0), followed by endocrinology (126.4) and family medicine/internal medicine (103.0). All other prescribing specialties fell below the average, with pediatrics being the lowest (62.0).
There were also some notable variations in year-over-year data (Fig. 6). PDOT for the family practice/internal medicine specialty (the largest specialty by prescribing volume) continued to increase from 2016 to 2017 (from 102.6 to 103.0), which was on top of a considerable jump (100.7 to 102.6) seen from 2015 to 2016. Cardiology saw a steady improvement over the three-year period from 2015 to 2016 (134.4 to 138.2, or 2.6 percent) and another 2.09 percent from 2016 to 2017 (138.2 to 141.1). PDOT for products prescribed by Pulmonary Disease specialists increased over the three years, with a greater increase between 2016 to 2017 (92.2 to 96.7, 4.86 percent).
In contrast, PDOT in the gastroenterology category dropped slightly from 2015 to 2016 (from 80.8 to 80.4, or -0.55 percent), and then dropped further from 2016 to 2017 (from 80.4 to 77.8, or -3.22 percent). PDOT in the emergency medicine category showed a decline from 84.9 in 2016 to 82.5 (-2.78 percent) in 2017.
Copays remain influential
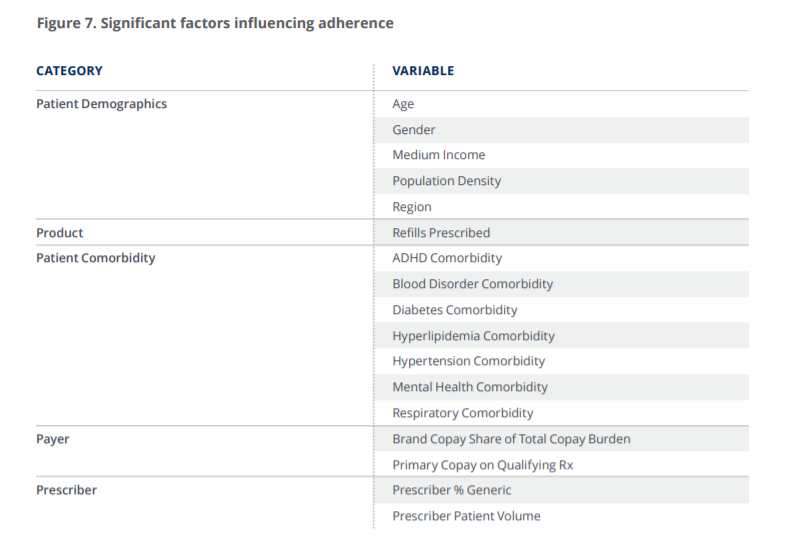
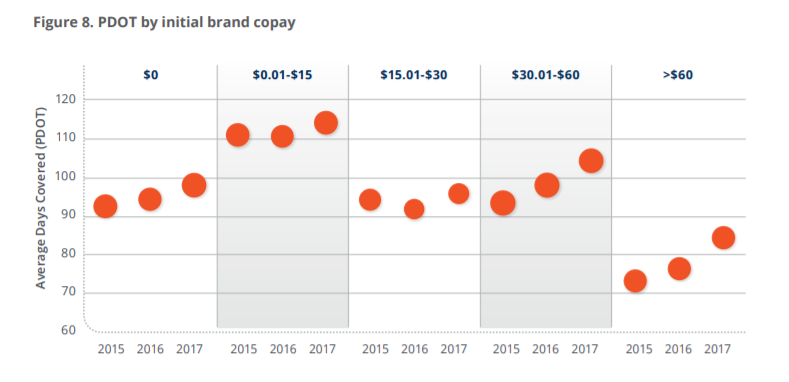
Since we began collecting this data in 2015, the top 15 factors influencing adherence have remained consistent (Fig. 7), and the patient copay is still the most influential factor overall. Each year we have found that, in general, higher copays lead to lower consumption of branded drugs (with the exception of $0 copays, which we found do not automatically lead to maximum consumption). Copays in the range of $.01-$15 (at 113.9 PDOT in 2017) still yield the highest rates of adherence.
However, consistent with our finding that overall PDOT rates are improving, we found that PDOT has been rising year-over-year in each copay category—even in the higher ones (Fig. 8). In fact, PDOT in both the $30.01-$60 and the $60 and higher copay ranges have improved more significantly than PDOT in the below $30 copay ranges. Digging deeper to understand why this might be the case, we did not observe any significant change in the underlying demographics—the number of patients, the overall trend and drug distribution by brand all remained constant. Nor were there new drug entrants or exits that would explain increasing rates of compliance at higher copay ranges. It is our theory that when someone is paying higher copays for their therapy and are actually staying on therapy, it is an indication that they are already committed to a healthier lifestyle and more likely to respond to other prompts reinforcing adherence and validating their behavior (e.g., dialogue with their physician, mobile apps, refill reminders, etc.).
Refills matter
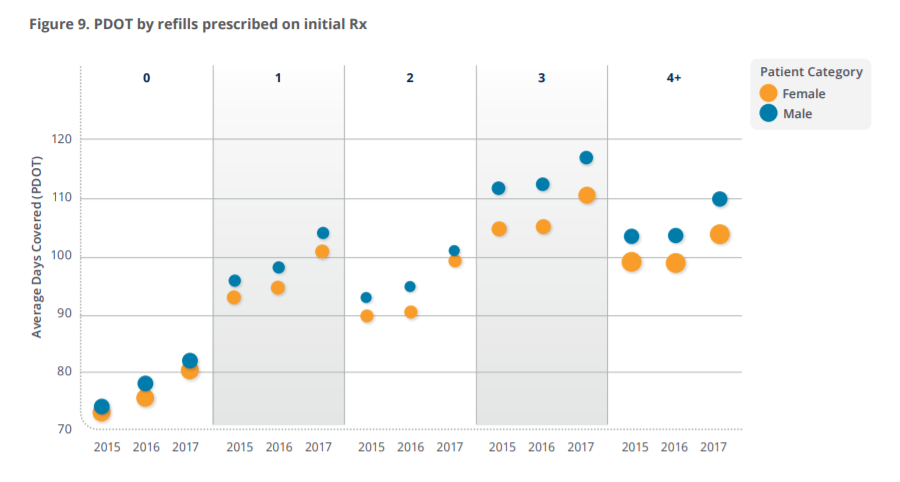
We have previously shown that a drug with even just one authorized refill is associated with an increase in PDOT of 20 days, and that in fact it does as much for consumption as bringing the copay down to $0.8 In 2017, we again found the impact of refills has a significant effect on adherence—an effect that increases along with the number of automatic refills authorized (Fig. 9).
Gender differences are also evident here. In every refill category, PDOT for men has climbed from 2015 to 2017 and has been consistently higher than for women. When we look at the behaviors of women among the same refill categories, we see one anomaly in the year 2016 where the trend is not as high for compliance; yet in 2017, women seem to catch back up in slope.
Concluding Thoughts: Building on Progress
The importance of medication adherence in ensuring effectiveness of pharmacological treatment has been discussed extensively and is widely accepted. Possibly one of the easiest ways to reduce medical costs while improving clinical outcomes is for patients to adhere to already prescribed therapies.
This report, the second in an annual series, looked at health behaviors through a specific lens—patients’ prescription refill behavior at the retail pharmacy. With the benefit of three years’ worth of data available to us now, we found some slow but steady improvement in adherence rates as measured by PDOT—a positive sign that concentrated efforts to improve adherence using the full range of both traditional tools (refill reminders, phone calls) and new digital and technological capabilities at our disposal may be making some headway toward improving medication adherence in chronic diseases.
Beyond the incremental change being facilitated by the current and emerging tools at our disposal, a major step that industry can take is to consider product features, patient adherence strategies and what evidence is needed to link these to outcomes much earlier in the drug development cycle. As we observe evidence of our population becoming more compliant to chronic prescribed medicine, the question is how this will play out in the form of overall patient outcomes, health and healthcare costs. Linking patient outcomes to prescription behavior may unlock the secret to better health.
References
1. Brown MT, Bussell JK. Medication adherence: WHO cares? Mayo Clinic Proc. 2011;86(4):304-314.
2. Varshnaya A. Medication non-adherence: A $290 billion unnecessary expenditure. The HealthWorks Collective.
Posted 2015年4月13日. Available at: https://www.triple-tree.com/strategic-insights/2015/april/medication-nonadherence-a-$290-billion-unnecessa/
3. Oswald, K. Non-adherence: medicine’s weakest link. Pharm J. 2018. Available at: https://www.
pharmaceutical-journal.com/news-and-analysis/features/non-adherence-medicines-weakest-link/20204378.
fullarticle?firstPass=false Accessed 10/15/18.
4. Kim J. Combs K, Downs J, Tillman F. Medication adherence: the elephant in the room. US Pharm.2018;43(1)30-34.
5. Nieuwlaat R, Wilczynski N, Navarro T, et al. Interventions for enhancing medication adherence. Cochrane Database
Syst Rev. 2014 Nov 20;(11):CD000011. doi: 10.1002/14651858.CD000011.pub4
Available at: https://www.ncbi.nlm.nih.gov/pubmed/25412402
6. Fischer MA, Stedman MR, Lii J, et al. Primary medication non-adherence: analysis of 195,930 electronic
prescriptions. J Gen Intern Med. 2010;25(4):284-290.
7. Hubbard TE. Ready for pick-up: reducing primary medication non-adherence: a new prescription for health care
Improvement. A NEHI Issue Brief. October 2014. Available at: http://www.nehi.net/writable/publication_files/file/
pmn_issue_brief_10_14_formatted_final.pdf
8. Stewart J, Morini L, Occhipinti M. Crossing the finish line: factors driving patient adherence to drug therapy: 2017年
patient adherence influence report. Syneos Health. Available at https://www.syneoshealth.com/perspectives/
crossing-finish-line-factors-driving-patient-adherence-drug-therapy
